In the last few years I have noticed Urgent Care Centers popping up in every town and city. These places are supposed to be an alternative to an Emergency Room visit: quick, easy and cheap (for the insurance companies). Insurance companies are promoting these places because an ER visit will cost 5 times more than an office visit, and if the insurance company can save thousands of dollars for one visit, they are all for it. It also is an alternative to a visit to our pediatric office because it offers “no waiting” and evening hours. Why wait 3 hours when your child can be seen now?
Unfortunately, in my experience with my patients, I have found that these Urgent Care centers are not what they are advertised to be, and are instead giving shoddy health care which, in the end, cause more problems then it helps.
Let me list my gripes:
-
Misdiagnoses by non-pediatric doctors:
These places are not staffed with pediatricians, but often are ER doctors with limited child experience. Sometimes nurse practitioners or physician assistants with little or no oversight of their work. I have seen in my office more than half of the “ear infections” to be false, pneumonias diagnosed as asthma or vice versa. They are ill qualified for pediatric work.
-
Over-prescribed and inappropriately prescribed antibiotics:
The joke in my office is that anytime a patient of mine went to an Urgent Care, I guess correctly that they got zithromax (azithromycin). It seems that every patient I see on follow up got this “wide spectrum” antibiotic. And, yes, there are situations to use this medication, it is inappropriate to use this “big guns” medication for ear infections and strep throat. (Hint: Penicillin/Amoxicillin is the first choice).
Secondly on this point, every cold with sinus pressure is not a sinus infection, and every cold with ear pain is not an ear infection. Nasal mucus will fill the sinuses and middle ear space many times during a viral infection and cause pain. But a BACTERIAL infection, secondary to the viral infection of these areas take time, usually 5-7 days.
Listen: sudden onset of ear pain in your child in the middle of the night at the beginning of a cold is usually just nasal mucus that dripped into the middle ear from the throat thru the eustachian tube. At-home management of this should be: sit up, take ibuprofen, drink water, take a steam shower, and maybe even Vicks. Zithromax at 3 am is not going to fix the problem or the pain.
“Then why does the Urgent Care provider say my child has an ear infection and gives me a prescription?” Because you, the parent, want something done and immediate satisfaction is the goal of these clinics. Their goal is to have you walk out of their office happy, not appropriately treated. (Sorry, it’s the truth).
-
Over-prescribed oral steroids:
This makes no sense to me. I have found that many of my patients received steroids for sore throats, cough, back pain, ear pain, and even headaches. This is criminal in my opinion. Steroids are very very serious medicine. (I’m not talking about anabolic steroids to increase testosterone levels, but corticosteroids that help with inflammation.) They should be used with the utmost caution. Your body makes natural steroids and maintains a small and consistent production by the adrenal glands. Doctors use steroids at 100 times the normal body level to suppress inflammation as it occurs in asthma and lung disease, or in severe allergic reactions such as from foods, drugs, or poison ivy contact. The dangers of steroids are many, including eye damage (cataracts), weight gain and obesity, hypertension, osteoporosis; and long-term use can damage any major organ in the body: liver, kidneys, heart or the brain.
I find these days that almost every patient that visited an Urgent Care is getting a prescription for steroids for basic symptoms like sore throat and pain. Some of these patients are very young and do not need steroids. The vast majority of swelling and inflammation can be treated with over-the-counter medications like ibuprofen or acetaminophen.
-
No follow-up or correspondence
When we send a patient to a sub-specialist or to the Emergency Room, we expect a full report of what happened. When a patient gets treatment for a disease or injury, we as primary care physicians want to know what happened and what needs to happen next in our patient’s care. That’s our job.
We do not have a partnership with the Urgent Care centers. They have no vested interest in following up with patient outcomes. When we call for reports or lab results, we are told its a HIPAA violation unless the patient has given written requests.
They are not interested in communication with us because we are the competition for their patients. They are open during the same hours we are, and do not feel a relationship is necessary.
-
Bogus diagnoses:
I said it. I think some of the professionals that work at these Urgent Care clinics are lying about their diagnoses. I think they look in an ear and say “oh, an ear infection,” when the eardrum (tympanic membrane) is clear. I think they listen to the lungs and say, “oh, pneumonia” when they hear nothing. I think they do a rapid strep test on and have a negative result but tell the patient “it is positive for strep.” I think they do a urine analysis test on a clean urine and say “oh, you have a urine infection.”
Why do I think this?
Because I have seen it.
I have had patients follow up with me in less than 24 hrs of visiting these clinics and they have nothing wrong. Their repeat rapid and urine tests are negative. Their ear and lung exams are clear. I have had patients who had a mistrusting experience with the clinic and saw me the next morning without taking the prescribed medication and shown me this.
Why are they doing this?
Because, as I said, their goal is to provide satisfaction, not good patient care. They are interested in the bottom line and that is influenced by patients getting what they want. And what parents and patients want are not always what they need. Studies show patients feel satisfied when they walk out of a doctor’s office with a prescription for something. That’s why they went to the office, to get something to fix their problem. What they need, however, is a doctor to figure out if they have something dangerous, using their experience and knowledge, and providing proper treatment for infection, injuries and symptoms that does no harm.
“So,” you are thinking, “What am I supposed to do?”
Well, at Fairview Pediatrics, we do have office hours from 8 am to 7 pm on most days. We have hours on Saturdays from 9 to 12. And we are soon to start beta testing walk-in hours from 8 to 9. We arrange our schedules to allow for parents and patients to call and get an appointment that day. Many adult providers and sub specialists make patients wait weeks to months before being seen.
“Well, what about after those hours?”
We have a nurse phone triage system that is there to help you decide one of three options:
- Can it be treated at home,
- can it wait until the next day,
- or does it need to be seen right away at the emergency room?
This system has worked for many years, and it still is working.
The draw of an Urgent Care is that the service appears instantaneous. Quick in and out with a prescription for your suffering.
The truth of the matter is that the Urgent Care business is simply a business to give people what they want regardless of their actual health care needs. It might be more convenient to walk into these places without taking time from work or your busy schedule, but it is not quality care. We are invested in your long term health needs, whether you want to hear it or not! Please consider your health care carefully and call us when you need us. We are in it for the long haul.
Thanks,
Dr. Jamie Bell
These days we do not lose our children to infectious diseases in the United States. Other third world countries do, but not us. Right?
I have seen a change in medicine from my childhood in the 70’s and 80’s, to medical school in the 90’s, to my practice of pediatrics in the 00’s and 10’s. I missed getting a smallpox vaccine when I was born in 1969. I got chicken pox in 1975 and had only a few spots. I got a booster vaccine during a measles outbreak in 1986. I had a pneumonia in 1987. Other than that, I did fine.
I saw diseases in medical school that we do not see much of anymore, like chicken pox, hepatitis B, and mumps.
In Pediatric residency in the late 90s we didn’t worry about Hib sepsis or meningitis, but were scared of pneumococcal meningitis in infants and menigococcal meningitis in teens. We sadly admitted babies with rotavirus dehydration in the summer, and admitted pertussis babies to the intensive care for ventilation support.
In pediatrics practice over the last 15 years I have seen a remarkable decrease in ear infections (thanks to the Prevnar vaccine for pneumococcus), decrease in rotavirus dehydration, and we have now started vaccinating children to prevent cancer.
It almost seems easy to raise children without the fear of infection these days. But these diseases are still out there in the world. They are waiting to come back.
What follows is a run down of all the diseases we routinely vaccinate again in our offices. If enough parents choose to delay, breakup, or outright refuse certain vaccinations, these diseases will come back to the United States.
These pictures are graphic, so please view at your own risk.
All statistics and facts were taken from the Center for Disease Control and Prevention, the World Health Organization, or the American Academy of Pediatrics sites. I have listed links to their web sites for further study.
Diphtheria:
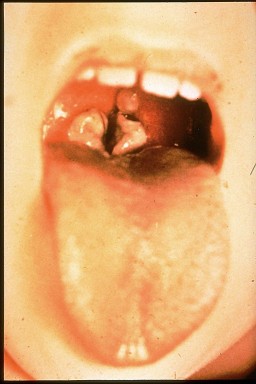 Bacteria, releasing toxin
Bacteria, releasing toxin- Symptoms: sore throat, fever, swollen tonsils
- Complications: myocarditis (heart inflammation), peripheral neuropathy (damaging nerves for sensation and movement)
- Death/Statistics: 5-10% of infected, by heart failure or suffocating from throat obstruction.
- In the USSR in 1998, there were 200,000 cases, and 5,000 deaths
- In its early stages, diphtheria can be mistaken for a bad sore throat. A low-grade fever and swollen neck glands are the other early symptoms.
- The toxin, or poison, caused by the bacteria can lead to a thick coating (or membrane) in the nose, throat, or airway. This coating is usually fuzzy gray or black and can cause breathing problems and difficulty in swallowing.
- Those infected have difficulty breathing or swallowing, even show signs of going into shock (skin that’s pale and cold, rapid heartbeat, sweating, and an anxious appearance).
- In cases that progress beyond a throat infection, diphtheria toxin spreads through the bloodstream and can lead to potentially life-threatening complications that affect other organs, such as the heart and kidneys. The toxin can cause damage to the heart that affects its ability to pump blood or the kidneys’ ability to clear wastes. It also can cause nerve damage, eventually leading to paralysis.
- Up to 40% to 50% of those who don’t get treated can die.
Tetanus:

 Bacteria, Clostridium tetani, releasing a toxin, “stepping on rusty nail”
Bacteria, Clostridium tetani, releasing a toxin, “stepping on rusty nail”- Symptoms: muscle spasms of neck, back, jaw,
- Complications: neonatal tetanus, (from un-immunized mothers, unhealed umbilical stumps), muscle spasms can break bones, brain damage, and cerebral palsy.
- Death/Statistics: from respiratory failure (lungs unable to expand) or cardiac arrest (heart stops)
- In 1998 in developing countries, 14% (215,000) of all newborn deaths.
- Tetanus is a serious bacterial disease that affects your nervous system, leading to painful muscle contractions, particularly of your jaw and neck muscles. Tetanus can interfere with your ability to breathe and, ultimately, threaten your life. Tetanus is commonly known as “lockjaw.”
- There’s no cure for tetanus. Treatment focuses on managing complications until the effects of the tetanus toxin resolve. Fatality is highest in individuals who haven’t been immunized and in older adults with inadequate immunization
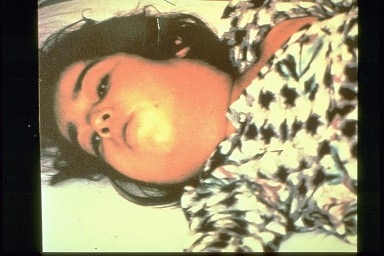
Pertussis:

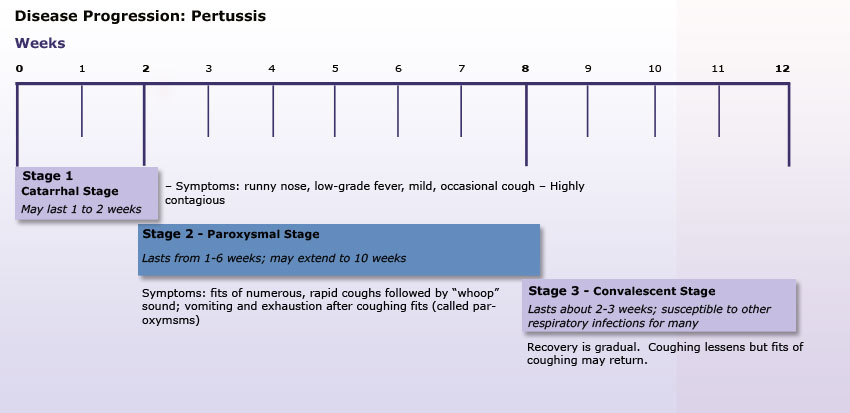 “Whooping Cough”, Bordetella Pertussis bacteria, from respiratory droplets
“Whooping Cough”, Bordetella Pertussis bacteria, from respiratory droplets- Symptoms: cold symptoms for 1-2 weeks, followed by overwhelming cough, sometimes vomiting, causing death in infants from suffocation, apnea
- Complications: pneumonia, convulsions, encephalopathy (infection of the brain)
- Death/Statistics: death rates of 1.6% in America, 4% globally. 48.5 million cases annually worldwide, and 295,000 deaths.
- This is not a disease from a foreign country. This disease is here, in Massachusetts, in the Pioneer Valley.Read the sad tale of Brady Alcaide from Chicopee, who died at 6 weeks of age in 2012. Too young to get the vaccine.
- Brady’s Story
- Pertussis is a bacteria that you can treat with antibiotics if you catch it early enough. After the first 2 weeks of the “cold symptoms”, however, any antibiotic treatment only prevents its spread, it does not stop the deadly “whoop” cough. This cough can last for months.
Polio:
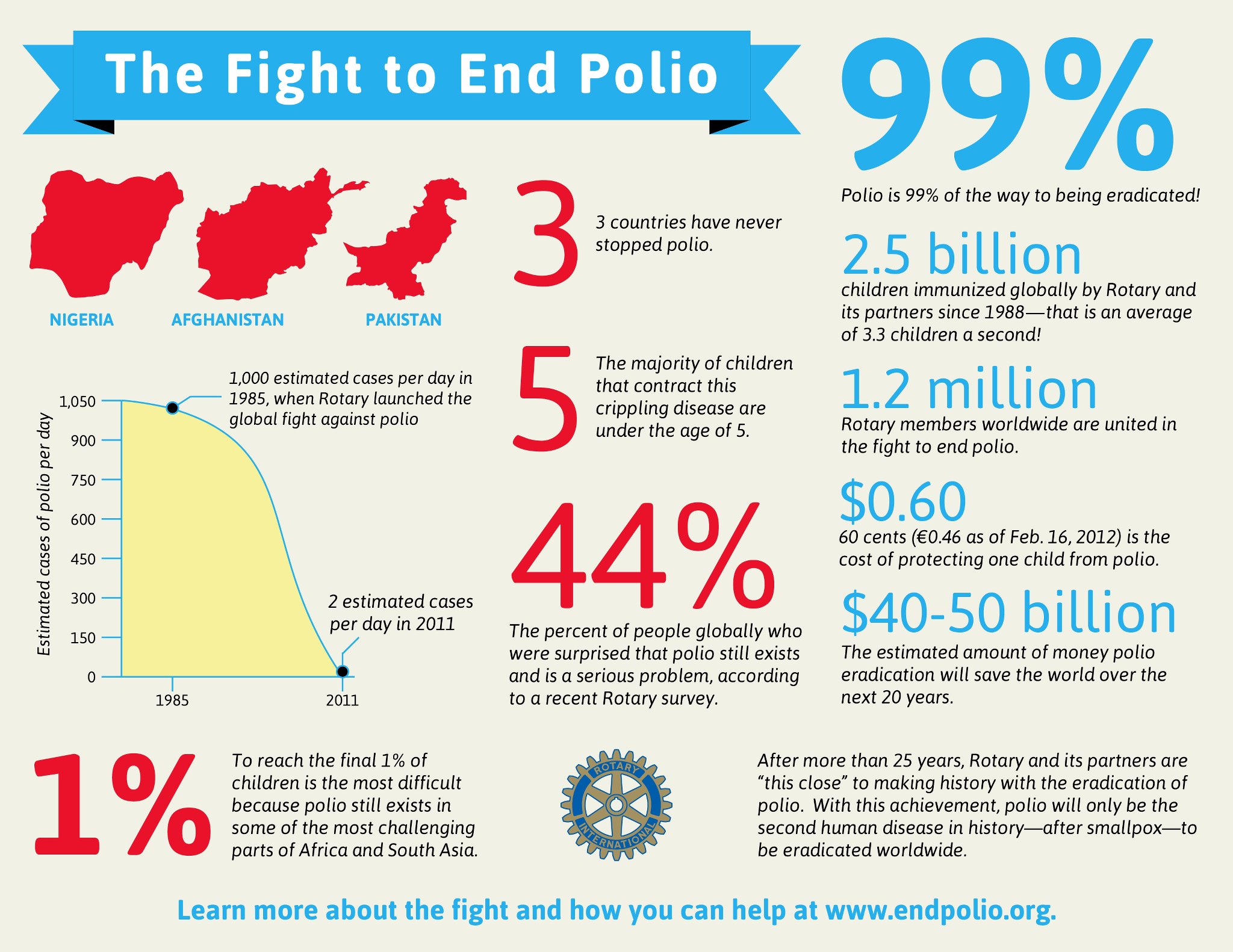
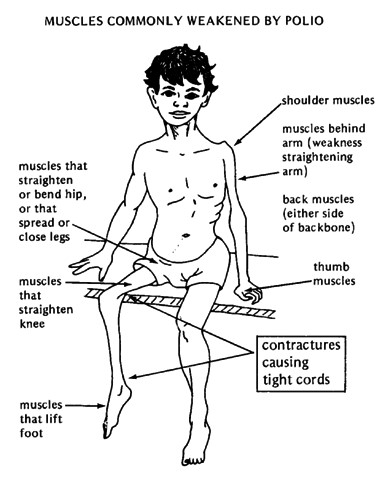 Virus, from infected food or water
Virus, from infected food or water- Symptoms: fever, headache, vomiting, stiffness
- Complications: 1% of infected develop muscle weakness in legs, neck, head or diaphragm, meningitis (infection of spinal cord and/or brain)
- Deaths/Statistics: 2-10% of those with paralysis die from suffocation because of diaphragm muscle paralysis, making them unable to breathe.
- Thanks to vaccines, polio cases dropped from 350,000 in 1988 down to on 416 cases in 2013, spreading in the countries of Afghanistan, Nigeria and Pakistan.
- There is no cure for polio, it can only be prevented.
- It mainly affects children under 5 years of age.
Hepatitis B
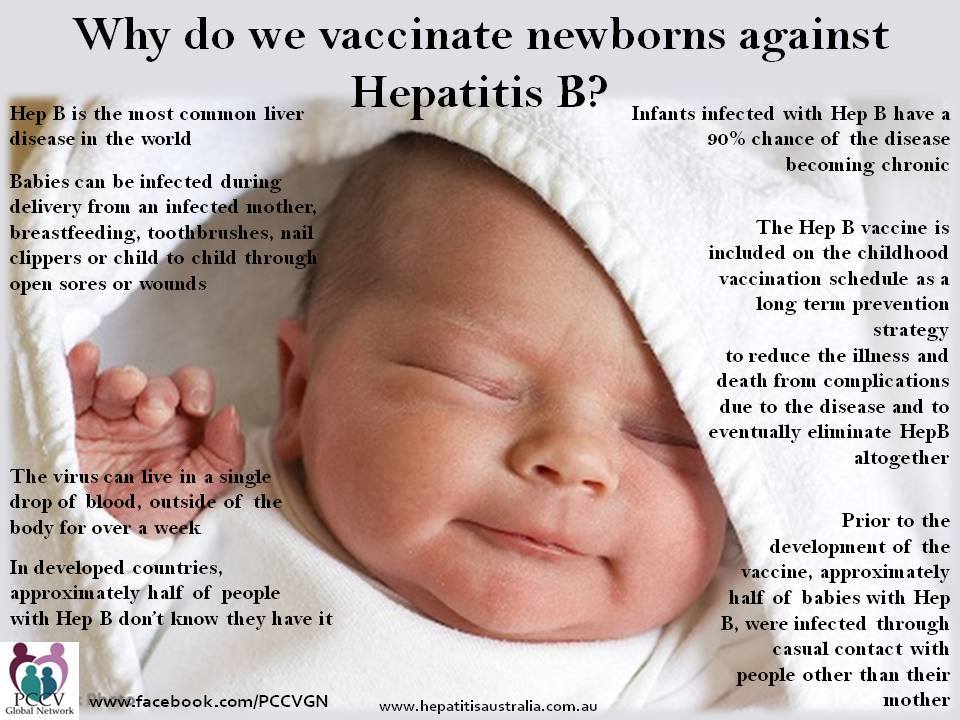
 Virus, infected blood (survives outside body for 7 days)
Virus, infected blood (survives outside body for 7 days)- Symptoms: fever, fatigue, loss of appetite, nausea, vomiting, jaundice (yellowing skin)
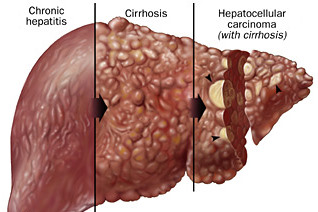
- Complications: scarring of the liver, cirrhosis, cancer
- Deaths/Statistics: in 2007, 43,000 new infections in the US,
- 800,000 to 1.4 million have chronic hepatitis B virus infection, 30-40% of these infections were acquired during childhood
- Globally, chronic Hep B affects 350 million people, contributes to an estimated 620,000 deaths worldwide each year.
- Hepatitis B is a contagious liver disease that ranges in severity from a mild illness lasting a few weeks to a serious, lifelong illness. It results from infection with the Hepatitis B virus. Hepatitis B can be either “acute” or “chronic.”
- Acute Hepatitis B virus infection is a short-term illness that occurs within the first 6 months after someone is exposed to the Hepatitis B virus. Chronic Hepatitis B virus infection is a long-term illness that occurs when the Hepatitis B virus remains in a person’s body.
- It is true that hepatitis can be acquired from sexual intercourse and shared needles. So why immunize infants and children? Because infection can occur from any blood contact, whether at birth or other exposures.
- 90% of infants who are infected will ultimately develop chronic hepatitis. Only 30% of children age 1-5 develop chronic hepatitis, and only 5-10% of healthy adults who are infected will develop chronic infection.
Hib/Haemophilus influenza (or “Hib”)

 Bacteria, respiratory droplets
Bacteria, respiratory droplets- Symptoms: causes ear infections, cellulitis (skin infections), infectious arthritis (joint infections), bacteremia (blood infections), epiglottitis (inflammation of the windpipe, like diphtheria), and meningitis (infection of the covering of the brain and spinal cord, stiff neck, fever, photophobia, confusion)
- Complications: meningitis resulting in coma or death
- Deaths/Statistics: before the vaccine, in 1992 there were 20,000 US children under age of 5 with severe infection, with 1,000 deaths, or about 3-6% of those infected.
- Before the vaccine, Hib disease was the leading cause of bacterial meningitis among children under 5 years of age.
- Although antibiotics can kill Hib, infected infants can have no symptoms to sudden fever, coma and death within hours.
- Delaying vaccination for Hib only allows more time for a young infant to be infected and killed by this bacteria in those early months.
- This bacteria is in the US. In fact, there is a good chance it is dormant in your nasal passages!
Pneumococcus
 Bacteria, respiratory droplets
Bacteria, respiratory droplets- Symptoms: Sudden onset of fever and fatigue, cough, pleuritic chest pain, blood-tinged sputum. Pneumococcal meningitis may present as a stiff neck, headache, lethargy, or seizures.
- Complications: similar to Hib, ear infections, cellulitis (skin infections), infectious arthritis (joint infections), bacteremia (blood infections), meningitis (stiff neck, fever, photophobia, confusion)
- Deaths/Statistics: 900,000 Americans get pneumooccal pneumonia each year and 5-7% die from it. There were 3,300 deaths in the U.S. from pneumococcal meningitis and bacteremia in 2012. About 3,000 cases of pneumococcal meningitis occur each year and of those cases 10% will die from the infertion.
- Pneumococcus is the most common cause of bloodstream infections, pneumonia, meningitis, and middle ear infections in young children.
- As Hib, antibiotics can kill pneumococcus, but infants are highly susceptible and can be asymptomatic, developing fever to death in a matter of hours.
- I can’t emphasize this enough, there is no time to save a baby from Hib and pneumococcal bacteremia or meningitis. I have seen a baby in the nursery seem fine at 9 am and in a coma at 12 noon.
Rotavirus
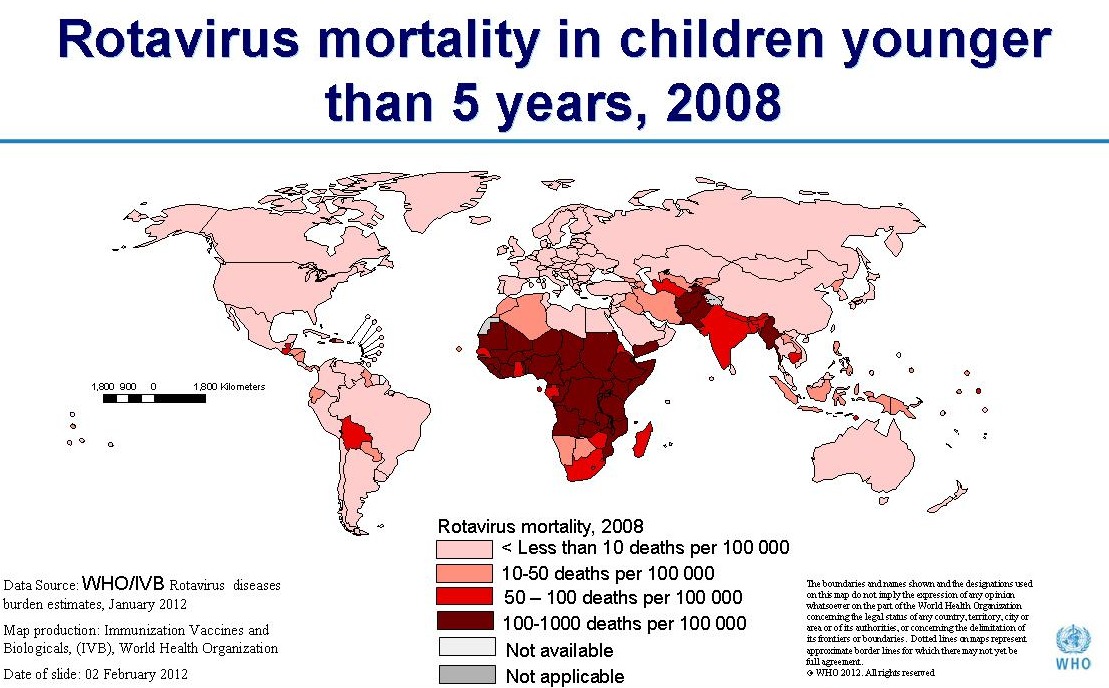
 Virus, fecal/oral transmission, contaminated water, food, surfaces
Virus, fecal/oral transmission, contaminated water, food, surfaces- Symptoms: diarrhea, vomiting,
- Complications: dehydration, sometimes severe resulting in cardiac arrest, sepsis, and death.
- Deaths/Statistics: before widespread vaccination, caused between 55,000 and 70,000 baby hospitalizations, and 20-60 deaths annually in the US.
- In 2008 worldwide, there were 453,000 deaths in children younger than 5 years of age due to rotavirus infections.
- As a virus, there is no treatment other than support through oral rehydration or IV fluids.
- Infants under 6 months of age are highly susceptible to rapid dehydration, and could be life threatening in hours.
Measles

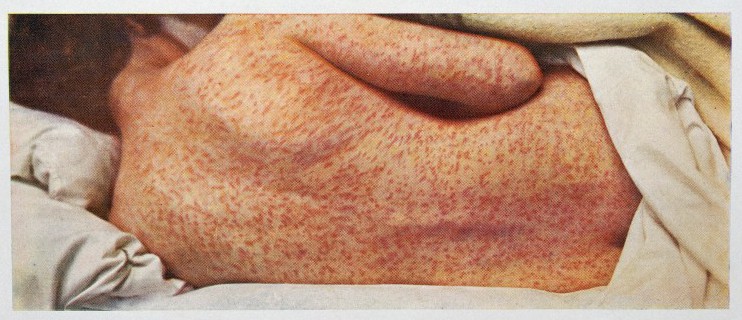 World Health Organization on measles
World Health Organization on measles- Kids’ Health on measles
- Virus, respiratory droplets, highly contagious
- Symptoms: fever (over 104), cough, runny nose, conjunctivitis (red eyes), red flat rash starting on the face, and spreading down the body.
- Complications: common complications such as ear infections and diarrhea, to severe complications of pneumonia or encephalitis.
- Death/statistics: 1 in 20 children develop pneumonia, 1 in 1000 children develop encephalitis, swelling of the brain that can cause seizures, deafness or mental retardation if it is survived.
- In the U.S., before vaccination in 1963, there were 3 to 4 million cases of measles each year. Of those people, 400 to 500 died, 48,000 were hospitalized, and 4,000 developed encephalitis.
- Worldwide, in 2013, there were 145,700 deaths.
- “400 deaths a day, 16 deaths an hour.”
- Before widespread vaccination, measles caused an estimated 2.6 million deaths each year.
- Measles was considered eliminated from the United States in 2000. That is, there were no transmitted cases between residents of the US.
- One dose of measles vaccine is about 93% effective, and two doses are about 97% effective.
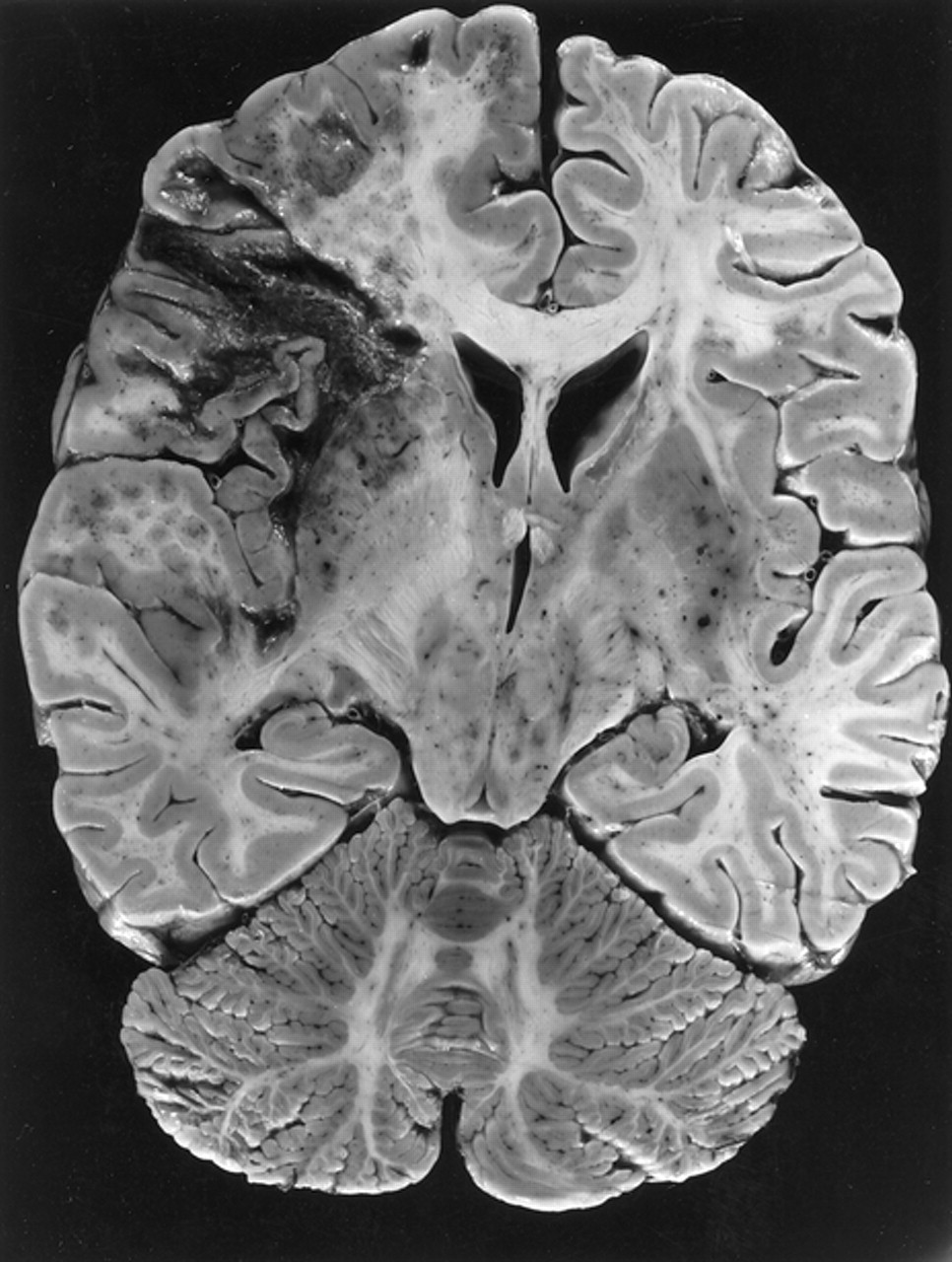
Mumps

 Virus, respiratory droplets
Virus, respiratory droplets- Symptoms: fever, headache, muscle aches, fatigue, parotitis – swollen and tender salivary glands under the ears or jaw
- Complications: inflammation of the testicles (orchitis) leading to atrophy and possible sterility. inflammation of the brain or meninges (encephalitits and meningitis), inflammation of the ovaries (oophoritis), deafness.
- Deaths/Statistics: symptomatic meningitis (headache and stiff neck) occurs in up to 15% of patients. Orchitis occurs in up to 50% of males. Encephalitis occurs in 2 per 100,000 cases. Deafness occurs in 1 of 20,000 cases. An average of one death from mumps per year was reported during 1980-1999.
- There is no specific treatment for mumps, only supportive measures.
- Before vaccination, was responsible for 10% of viral meningitis in the United States.
- Was the most common cause of sensorineural deafness in childhood.
Rubella

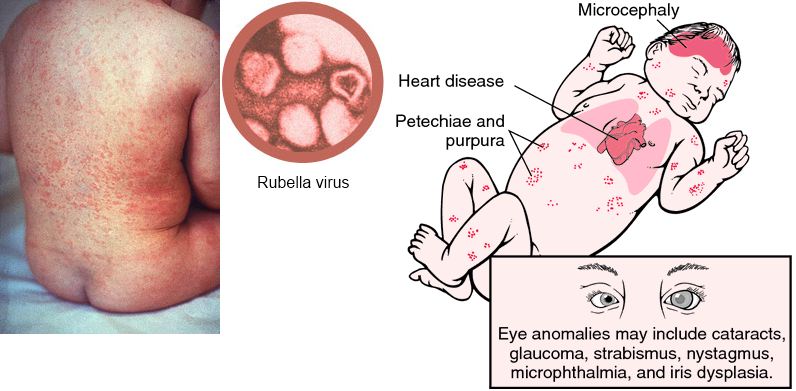 “German Measles”, virus
“German Measles”, virus- Symptoms: low grade fever, tender lymph nodes, rash on face that spreads down body
- Complications: in pregnant women causes Congenital Rubella Syndrome (CRS), born with growth and mental retardation, heart defects, eye defects (such as cataracts), deafness, liver, spleen and bone marrow complications.
- Death/Statistics: 20% chance of damage to the fetus if a mother is infected early in pregnancy. During the 1962-1965 global rubella pandemic, an estimated 12.5 million rubella cases occurred in the United States, resulting in 2,000 cases of encephalitis, 11,250 therapeutic or spontaneous abortions, 2,100 neonatal deaths, and 20,000 infants born with CRS.
- Although Rubella has been eliminated in the United States, it is endemic in the rest of the world, responsible for an estimated 100,000 infants born with Congenital Rubella Syndrome each year.
Varicella/Chicken Pox

 Virus, very contagious
Virus, very contagious- Symptoms: fever, fatigue, itchy, blister-like rash
- Complications: dehydration, pneumonia, encephalitis, sepsis, toxic shock syndrome, bone and joint infections.
- Deaths/Statistics: until nationwide vaccinations in the 1990s, an average 4 million people got varicella, 10 to 13,000 were hospitalized, and 100 to 150 died each year. The highest rate of varicella was in preschool aged children.
- Although most cases are mild, scarring can be severe, and other skin complications will last a lifetime.
- In my medical school years I saw a preschooler with varicella pneumonitis, or chicken pox pneumonia, which would lead to scarring of the lungs. (You could see the pox marks on her chest x-ray.) I also saw varicella encephalitis in a grade school boy who miraculously woke from his coma without lasting neurological damage.
- Those medical school experiences taught me that even though it was rare, it was very real to those parents, and there was the very real possibility of them losing their child to this virus.
Meningococcus
 Bacteria, Neisseria meningitidis
Bacteria, Neisseria meningitidis- Symptoms: sudden onset of fever, headache, and stiff neck, also nausea, vomiting, photophobia, and confusion
- Complications: sepsis (bloodstream infection) meningitis
- Deaths/Statistics: 10-15% of cases are fatal, of patients who recover 11-19% have permanent hearing loss, mental retardation, or loss of limbs.
- Infants less than 1 year of age and adolescents aged 16 through 21 have the highest rate of disease.
- 10% of people have this bacteria in the back of their nose or throat with no signs or symptoms, they are carriers.
- I have seen a teenager who had a headache and fever in North Adams at his camp, given a shot of antibiotic but arrived at Baystate Hospital in full sepsis and full organ failure, eventually losing 3 limbs from gangrene necrosis.
Human Papilloma Virus
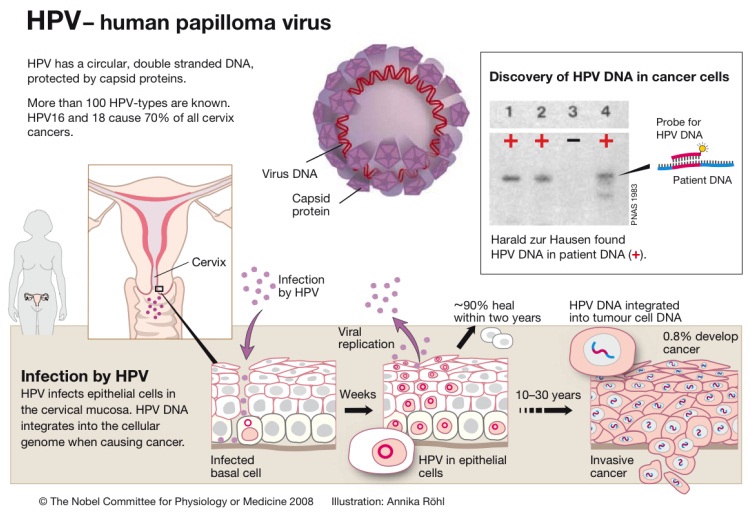 HPV – group of 150 related viruses, resulting in warts (papillomas)
HPV – group of 150 related viruses, resulting in warts (papillomas)
HPV is the most common sexually transmitted infection. HPV is a viral infection that can be spread from one person to another person through anal, vaginal, or oral sex, or through other close skin-to-skin touching during sexual activity. If you are sexually active you can get HPV, and nearly all sexually active people get infected with HPV at some point in their lives. HPV16 and HPV18 cause 70% of all cervical cancers.
As you can see, these diseases are still very common worldwide, but uncommon in the United States, thanks to the vaccine program developed over the last century. Within the Center for Disease Control, the Advisory Committee on Immunization Practices (ACIP) review and study vaccines, its efficacy and safety, with approval from American Academy of Pediatrics (AAP), the American Academy of Family Physicians (AAFP), and American College of Obstetricians and Gynecologists (ACOG).
It is my hope that this review of these diseases further informs you regarding the necessity of vaccines and universal vaccine coverage. My next blog will hope to explain in depth the safety of vaccines and its components.
 In my youth, exposure to pornography was limited to pictures in hidden Playboy magazines. Now, with a few clicks your son can visit websites of torture, rape, and further humiliation of women. Nowadays, a boy can stream videos in the privacy of his own room.
In my youth, exposure to pornography was limited to pictures in hidden Playboy magazines. Now, with a few clicks your son can visit websites of torture, rape, and further humiliation of women. Nowadays, a boy can stream videos in the privacy of his own room.
There is no proof that pornography leads to a criminal deviant mind, but it can teach a boy about sex and women. If you allow pornography to the the sex educator of your son, you risk teaching him that girls and women enjoy being sexually used, dominated and humiliated by men. Pornography will teach your son to objectify women, and treat them as toys for their own sexual gratification. Pornography does not teach tenderness, caring, or love. Without proper guidance, our boys will be overwhelmed with thoughts and ideas that degrade love and will not lead to lifelong fulfilling relationships.
Boys and girls grow and develop differently and at different ages. When is the best time to confront these issues? My guess is to start around 5th and 6th grade. These are the ages that children are curious about their sexuality and may start exploring. But, it is important to realize that sexuality and maturity changes thru the years, and our approach and tactics change with them.
Sadly, I have few recommendations regarding protecting our children from online graphic images. I have researched parental restrictions on my MacAir, Desktop Mac, iPad, and iPhone, and have found this to be increasingly frustrating. There are, however, steps that responsible parents should take to prevent their children from seeing graphic images, and to confront their children with the realities of love, sex, and relationships.
To prevent pornographic exposure:
-
Parental Controls:
Many children have iPhones these days. It can be a great convenience to be able to contact and locate your child at a moment’s notice. The price for this convenience is your child’s access to the World Wide Web anywhere and at any time.
Before giving your child a smart phone, set up the parental controls. It is easy enough on the iPhone and iPad: Settings > General > Restrictions > Enable Restrictions. Set a 4 digit Passcode. You can prevent your child from downloading apps, surfing the web, and doing FaceTime. Under “Allowed Content” you can restrict websites to Limit Adult Content or even restrict access to specific websites.
-
Restrict computers and phones to outside the bedroom and keep computers in “high traffic” areas.
When your child is alone in their room, you have no control over their use. Make this the law in the house. (the added benefit is cutting down on distractions like YouTube, Netflix, or simple web surfing during homework time!)
-
Review your child’s internet history
Make it the rule in the house to NOT clear internet histories. This is the honest way to see what your child is viewing online.
-
Monitor your child’s Facebook, Instagram, or other social network sites.
I believe it is not an invasion of privacy for parents to have access to their online conversations. This is important to see who your child is talking to, what they are talking about, and to see if your child is being solicited by older people.
-
Talk to your child.
This is the hardest one. We all have sexual thoughts. We do. As much as we want to deny this, our children will grow into sexual beings. As parents and adults we all have our hang-ups, and fears and avoidance issues. But this is a serious subject and important for our child’s development.
I have a friend who wrote a great letter to his son after he found evidence of him surfing pornographic sites. I recommend reading this, perhaps downloading it and giving it to your pre-teen son as a starting point for an honest discussion about sex, love, and relationships:
“Mark,
You will find that the computer is locked…and you know why. Yesterday is the second time—about which I am aware—that you have used the computer to surf the websites that I have told you not to visit.
You are doing well in school, you are getting your work done without much prompting, you are working hard at three sports, you are singing in the a cappella group and participating in student council, you are helping your seriously disabled coach and by all accounts you are being a good big brother and son. Mom and I are very proud of you and very happy with the way you have been exercising responsibility. Surfing porn does not erase all of that; it does not make you a bad person. Although it is perfectly normal to be curious and excited by pornography, it can be harmful to you.
It can be harmful because of the images and videos on the internet are distortions of reality. They depict women as objects and depict sex as some type of mistreatment of women. It is an unhealthy view of sex and relations between adults. Viewing this material as you are sexually maturing can affect the way you feel about and relate to women. This is not a question of choices you will later make in relationships, it is a question of conditioning your brain and affecting normal sexual arousal. You should be able to be sexually aroused at the thoughts of women or the mere appearance of them dressed seductively or in a state of undress. Sex is a mutual act of intimacy between two people; it is not something one person does to the other. By watching these images for sexual enjoyment, you will unwittingly condition yourself to this type of stimulation and it can affect your real life relationships with women at a later date.
I am not just forbidding you to watch hardcore pornography; I am also explaining why it is forbidden. I want you to understand that this can harm you. I know that it seems private and that no other people are involved, but there are other people involved. Women are sometimes abused and forced to perform in these videos—even if it looks like they are enjoying themselves. Also, when you go on a pornography website, you allow access into our computer from people outside of our home. You are not alone when you are on the internet. The people who provide this information know what you are looking at. These people cannot be trusted.
There is more to talk about and Mom and I need to discuss how to help you to understand and not do it again. I wish this stuff was not out there. When I was your age this stuff was only available to adults and they had to go to creepy stores to get it. I know it is tempting at your age to want to look at this stuff, but it is not good. I love you very much, and that is why it is so upsetting to me that you are exposed to this material.
Do your homework.
Love,
Dad”
This is what I have for now. Let me know if you have other ideas or thoughts on approaching young pre teens and teens with regards to sex, sexuality, and online viewing.
 “Why should I get the flu shot? I never get the flu.”
“Why should I get the flu shot? I never get the flu.”
“The flu shot gets you sick!”
“Only sick people die from the flu.”
I see a number of parents with children in the office who refuse to give their child a flu shot. The most common reason is “He’s never had the shot before, and he never has had the flu.”
Influenza, or the flu, comes around every year. It affects the youngest and oldest most severely, and it can be very difficult to treat. The best medical advice that I can recommend is to get the vaccine every year.
Still not convinced?
Here are a few points to remember regarding the flu, the vaccine, and doing your part for your community:
-
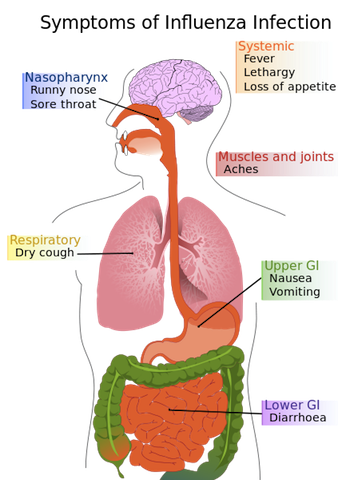
The “Flu” is not a “24 hour stomach bug” or “the stomach flu”
The influenza virus causes an upper respiratory infection with cough, congestion, runny nose, sore throat. Sometimes people can have headache, muscle aches, fatigue and fever. Vomiting and diarrhea does occur sometimes, but this is mostly in children. Symptoms start usually in 1-4 days of exposure, with an average of 2 days. Symptoms can last from a few days to two weeks. (CDC)
-
 “I never get the flu” is a false statement.
“I never get the flu” is a false statement.Fact is, you probably have had the flu before but did not realize it (see #1). In the US, on average 5% to 20% of the population get the flu.
Perhaps you had a “cold” with cough and sore throat for a week. Maybe you had a runny nose and felt tired in February last year. Everyone responds to the influenza virus differently with different symptoms, intensity and time course. Truth be told, almost everyone has had the flu at least one time in their lives. (CDC)
-
 There are many influenza viruses.
There are many influenza viruses.You may have heard of “bird flu” or “swine flu”, specifically H1N1, which had a pandemic outbreak in 2009.
Here is the CDC explanation for types of influenza viruses:
“There are three types of influenza viruses: A, B and C. Human influenza A and B viruses cause seasonal epidemics of disease almost every winter in the United States. The emergence of a new and very different influenza virus to infect people can cause an influenza pandemic. Influenza type C infections cause a mild respiratory illness and are not thought to cause epidemics.
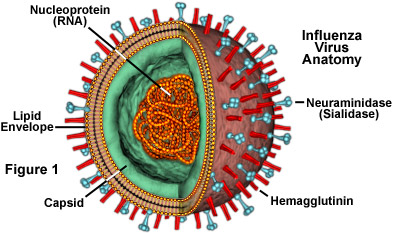
Influenza A viruses are divided into subtypes based on two proteins on the surface of the virus: the hemagglutinin (H) and the neuraminidase (N). There are 17 different hemagglutinin subtypes and 10 different neuraminidase subtypes. Influenza A viruses can be further broken down into different strains. Current subtypes of influenza A viruses found in people are influenza A (H1N1) and influenza A (H3N2) viruses. In the spring of 2009, a new influenza A (H1N1) virus (CDC 2009 H1N1 Flu website) emerged to cause illness in people. This virus was very different from regular human influenza A (H1N1) viruses and the new virus caused the first influenza pandemic in more than 40 years. That virus (often called “2009 H1N1”) has now mostly replaced the H1N1 virus that was previously circulating in humans.” (CDC)
This is why you can get the flu every year. There are many different combinations of the H and N types, such as H1N1, H3N2, etc. Your immune system may have learned to fight H1N2, but not H2N3, etc.
H1N1 cause the Spanish Flu. H3N2 caused the Hong Kong Flu in 1968. H2N2 caused the Asian Flu in 1957.
You may have had the flu in the past, but you can get it again every year. You may have had the vaccine in the past, but that does not count for this year.
Each year the CDC uses statistics and epidemiology studies to predict which strain is most likely to spread to nationwide infectivity. In the most recent years, the vaccine protects against 3 flu viruses: influenza A (H1N1), influenza A (H3N2), and an influenza B. This year, 2013, a vaccine against four viruses, (quadrivalent vaccine), includes an additional B virus.
-
The influenza infection can be deadly.
The infection is especially deadly to the elderly, children, and asthmatics. But this does not mean healthy people are at no risk. Sadly, my son’s best friend’s father died of influenza last year. He was healthy, and in his late 40s.
Viruses themselves do not usually cause death, but it is the complications from the disease that lead to death. The infection causes an increase in nasal mucus, which can drip into the lungs. The weakness and fatigue makes it difficult to cough out the mucus. This can lead to a bacteria pneumonia in the lungs. Vomiting and diarrhea can lead to dehydration which can lead to heart failure or kidney failure. If a child has underlying asthma, she may have more inflammation in her lungs. An elderly person may not have the strength to cough and may develop pneumonia this way.
-
The next Flu outbreak could be “The Big One.”
2009 was the outbreak of H1N1 “swine flu” and caused quite a scare. It is estimated that it caused up to 88 million cases of flu, and between 8,000-18,000 deaths that year.
It was nothing compared to the 1918 H1N1 Spanish flu pandemic, which infected 1/3 of the world population, or 500 million people, and killed an estimated 50-100 million people.
I do not want to be an alarmist, but the CDC cannot predict the future, and you cannot guess which year will have a more deadly flu strain. You cannot wait until there is a serious outbreak and expect to get your vaccine. (it takes at least 2 weeks to develop an immune response to the vaccine).
-
Maybe your daughter will not get very sick from the flu, and does not “need” the vaccine, but grandma does not need to catch it from her.
Perhaps this is the best reason to get the vaccine. The virus needs a host to infect and spread the disease to another host. The vaccine stops the spread of the disease. If everyone in the country got the vaccine, conceivably we could prevent yearly pandemics.
To put it bluntly, NOT getting the vaccine makes you and your child part of the problem and not the solution. For example, your teenager may get the flu, with simple congestion and sore throat for a week, but spread it to his classmates. One classmate who catches the flu gives it to his cousin on chemotherapy, or a newborn niece, or a young brother with asthma, or a elderly grandmother.
-
Antiviral medications are not very effective.
There is no cure for the common cold, nor is there an cure for influenza. There are antiviral medications like Tamiflu (oseltamivir) or Relenza (zanamivir) are not as effective as the drug companies would like you believe. Antiviral medications do not pack the “punch” like antibiotics on bacteria. Also, viruses seem to develop resistance to medications faster than bacteria.
Remember that drug resistance in viruses and bacteria works like Darwinian natural selection, where the susceptible viruses or bacteria are killed off, leaving behind only the resistant virus which grow and reproduce more drug resistant viruses and bacteria. The more we use antiviral medications the more we end up with resistant influenza viruses.
Anti-viral flu medication helps only if started in the first 48 hrs of onset of symptoms, and it is difficult to distinguish between colds and influenza in those first few days.
In most cases flu treatment is supportive – plenty of fluids and rest, giving the body and immune system the strength to fight it on its own.
-
The vaccine is safe as can be.
The flu vaccine does not give “the flu.” Your body may “think” it has the flu, and respond with as if it is sick, but it is not the real flu, and it is mild, if anything.
There can be side effects from vaccines, that is true. Your body may react like the vaccine is an allergen. The body may turn on a fever response to “burn out” the infection. The worst side effect documented and attributed to the vaccine is Guillain-Barre syndrome (GBS), which is an auto immune attack on peripheral nerves, usually causing temporary weakness and potential paralysis of lower extremities. The syndrome can last for weeks, and is at greatest risk when it affects the diaphragm muscles for breathing. That being said, the rate of vaccine related Guillain-Barre syndrome is low. The association was noted during the outbreak of swine flu in 1976.
A recent study in the Lancet journal demonstrated a low attributed risk from the vaccine:
“The attributable risks were 1.03 Guillain-Barré syndrome admissions per million vaccinations, compared with 17.2 Guillain-Barré syndrome admissions per million influenza-coded health-care encounters.”
In other words, you are more than 17 more likely to get GBS from the infection, than from the vaccine.
Again, everything we do has calculated risks. Driving in a car, trying new foods, crossing a bridge, etc. etc. But the vaccine is an insurance policy against the flu. The risks from side effects are very low, especially compared to the risk of getting the flu and its complications.
-
There is no controversy with flu vaccines.
The flu shot does not cause autism. The flu shot does not cause Alzheimer’s disease. There is no federal conspiracy regarding vaccines, and the pharmacutical companies are not just trying to make money on vaccines.
Remember that there are scientific studies on vaccines that have reviewed side effects of vaccines. There is true science and it is published in medical journals such as Pediatrics, New England Journal of Medicine, and Journal of the American Medical Association (JAMA).
Parents do not have to do research on their own other than checking with these verified journals, and the Center for Disease Control.
Research on the internet, blogs (ha!), or facebook can be hearsay, ancedotes, lies or conjecture. People can make claims of associations of vaccines and unknown diagnoses like autism and Alzheimer’s because the etiology of these disorders are not known.
For example: You can make associative claim that whole milk, when started at 1 year causes autism, because almost all children are started on milk at a year. Therefore, you can say, “Look! This child started milk and then got autism at 18 months!” That is guilt by association, and it is not science.
Another example: doing crossword puzzles cause Alzheimer’s because of the association. My paternal grandmother did crossword puzzles every day up until she developed the unfortunate signs of Alzheimer’s. A lot of elderly people do crossword puzzles. A lot of them develop Alzheimer’s. By this association one could claim crossword puzzles cause Alzheimer’s!
Can you prove that it doesn’t?
It is the fear of the unknown that have fostered these claims. It is sad, because parents who want the best for their child are being scared by facebook blogs about how “unnatural” shots are, and it is better to get the disease naturally, or that we are trying to trick parents into harming their children.
At some point you have to trust that the doctor has read the literature, and the CDC have done the studies to prove it. You must accept the safety of proven medication treatment and ignore the hysteria of conspiracy.
The point is that the threat of influenza is real, and it is dangerous. For most people the infection is manageable. It can mean lost school time or work and has a financial impact. The real dangers of influenza are the complications from influenza that causes serious disease in infants, children, and the elderly. This is real science and is proven fact.
The responsible parent protects their child from serious disease, and potential deadly disease. The responsible parent also protects their neighbors and extended family from disease by immunizing their children.
-
There are multiple ways of getting vaccinated from flu
In our office at Fairview Pediatrics we order vaccine from the state and private supplies. We offer single dose vials (Thimerosal free), of the trivalent and some quadrivalent flu vaccine. We also offer the live attenuated influenza vaccine, FluMist, which is given as a nasal spray. This can only be given to our patients over 2 years old, without history of asthma, or other chronic lung or heart condition, or have immunosuppression.
Children can receive their first flu vaccine at 6 months of age. During the child’s first flu season receiving the vaccine, it is advisable to get a second shot in 1 month to insure proper immune response and protection from the infection.
So, in summary:
- The flu is not a 24-hour stomach bug.
- “I never get the flu” is false. Almost everyone has had it.
- There are many types of flu, with different strains each year.
- Influenza infection can be deadly, even to normal healthy people.
- It is impossible to predict a bad season, so waiting to vaccinate may be too late.
- Your child may be healthy, but unvaccinated children are a risk to the elderly and vulnerable individuals.
- You cannot count on anti-viral medication to help if you are sick.
- The vaccine is safe.
- There is no controversy about the flu vaccine.
- There are options for vaccination.
As you may have noticed, the Centers for Disease Control, the CDC, is my best resource for factual information regarding influenza and the vaccine.
 My Irish grandmother from Staten Island, NY told me three stories in my childhood that influence my practice of pediatrics and position on vaccines. The first story was how her only brother died at 4 years of age from an ear infection (perhaps pneumococcus bacteria). The second story involved a boy down the street from her, in 1953?, who was healthy on a Tuesday and in an iron lung machine on a Thursday, eventually dying from paralysis due to polio. The last story was the day her mother gathered her 4 daughters around her to tell them the news of the Salk vaccine breakthrough, and they danced and cried tears of joy.
My Irish grandmother from Staten Island, NY told me three stories in my childhood that influence my practice of pediatrics and position on vaccines. The first story was how her only brother died at 4 years of age from an ear infection (perhaps pneumococcus bacteria). The second story involved a boy down the street from her, in 1953?, who was healthy on a Tuesday and in an iron lung machine on a Thursday, eventually dying from paralysis due to polio. The last story was the day her mother gathered her 4 daughters around her to tell them the news of the Salk vaccine breakthrough, and they danced and cried tears of joy.
Sadly, I do not have parents crying tears of joy when I give vaccines to their children. Quite often I am confronted with questions regarding the science and safety of these vaccines: “Why now?” “Why so many?” “Is this really necessary?” “Doesn’t that cause autism?”
To reassure parents, I have summarized my thoughts on these questions:
1. Many vaccine preventable diseases children contract are difficult or impossible to treat once contracted. For example, polio causes paralysis, measles causes neurological complications, including death.
2. Vaccines for serious diseases have been developed over the decades to prevent children from ever contracting these serious diseases. The Salk polio vaccine developed in 1952, when there were 58,000 cases that year. The measles vaccine was licensed in US in 1964, yet world wide caused 630,000 deaths in 1990.
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm4829a1.htm#fig1
3. Vaccines stimulate our immune system to recognize the disease virus or bacteria by developing memory antibodies, which will prevent the disease from ever entering the body.
http://www.healthychildren.org/English/safety-prevention/immunizations/pages/How-do-Vaccines-Work.aspx
4. All of these diseases are still around and causing outbreaks around the world. (diphtheria – Russia 1990-1993) (Polio outbreaks in Somalia, Kenya and Ethiopia in 2013)(8 outbreaks of Measles in the US from Jan to August in 2013). Smallpox, a deadly disease, is no longer around BECAUSE of everyone’s compliance with getting the vaccine.
http://www.cdc.gov/measles/outbreaks.html
5. Vaccines may have risks, but everything we do is a calculated risk. Driving children to school, eating food at a restaurant, taking a new medication, etc. The calculated risk of a child contracting and being impacted by meningitis, pertussis or measles is far greater than any real risk from the vaccine. There are documented possible side effects from vaccines, but the protective benefits significantly outweigh the potential risks.
http://www.cdc.gov/vaccines/vac-gen/side-effects.htm
6. There is too much false information about vaccines: myths, anecdotal stories, alarmist websites and outright lies regarding vaccines as the cause of autism or other issues. English “scientist” Wakefield set the stage for MMR controversy with his flawed study which has since been disproven:
.http://en.wikipedia.org/wiki/Andrew_Wakefield A good summary of the controversy
http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(97)11096-0/abstract The Lancet retraction.
http://pediatrics.aappublications.org/content/108/4/e58.short A study in American Academy of Pediatrics Journal disproving Wakefield
http://www2.aap.org/immunization/families/autismwakefield.html A better explanation of the controversy by the AAP.
7. The vaccine schedule was developed to protect infants and children from these diseases at the earilest possible ages. Epidemiological studies have been done to determine the best time to give the shots and how often to give them to provide the highest proportion of community protection. (We need a community with greater than 90% protection to prevent the given virus or bacteria from surviving in our population.
8. Vaccines are tested and verified by the Federal Drug Agency,( FDA), the Center for Disease Control (CDC) with the Advisory Committee on Immunization Practices, (ACIP), and US Department of Health and Human Services – National Institute of Health (NIH), and approved by the American Academy of Pediatrics (AAP)
AAP http://www2.aap.org/immunization/
CDC http://www.cdc.gov/vaccines/
ACIP http://www.cdc.gov/vaccines/acip/index.html
FDA http://www.fda.gov/BiologicsBloodVaccines/Vaccines/default.htm
NIH http://www.niaid.nih.gov/topics/vaccines/Pages/Default.aspx
The development of vaccines – “The History of Vaccines”
http://www.historyofvaccines.org/content/articles/vaccine-development-testing-and-regulation
Vaccines and “overwhelming the immune system”
http://www.cdc.gov/vaccinesafety/Vaccines/multiplevaccines.html
I hope this helps. Remember that as pediatric physicians, we have trained and studied to provide the best care and protection for your child. This does come down to a question of trust. Do you trust your doctor and science, backed up by years of documented studies, experience and experiments? Or do you believe something you read on a website with no scientific studies or verification?
We doctors give these vaccines to our own children, and we want the best for your child. Our creed is “Do No Harm.” There is no global conspiracy regarding vaccines. It is proven science. Delaying or changing the vaccine schedule for your child puts your child at more risk for disease, and puts every other child in our community at added risk.
A few other helpful links:
Vaccine Schedule: http://www.cdc.gov/vaccines/schedules/hcp/imz/child-adolescent.html
Top Parental Concerns: http://www.cdph.ca.gov/programs/immunize/Documents/IMM-917.pdf